Surgical Treatments for Parkinson's Disease:
The following are surgical options available for Parkinson's patients. None are cures, nor do they halt the progression of the disease but they do address the symptoms and can supplement pharmaceutical therapies.
Brain surgery is difficult because the CT or MRI images the doctor works with to navigate the brain are indicative of the moment when the images were taken. Once the surgeon enters the brain, the brain moves due to fluid changes. Also, any cut could cause one to lose function due to severing of a connection.
Deep Brain Stimulation (DBS):
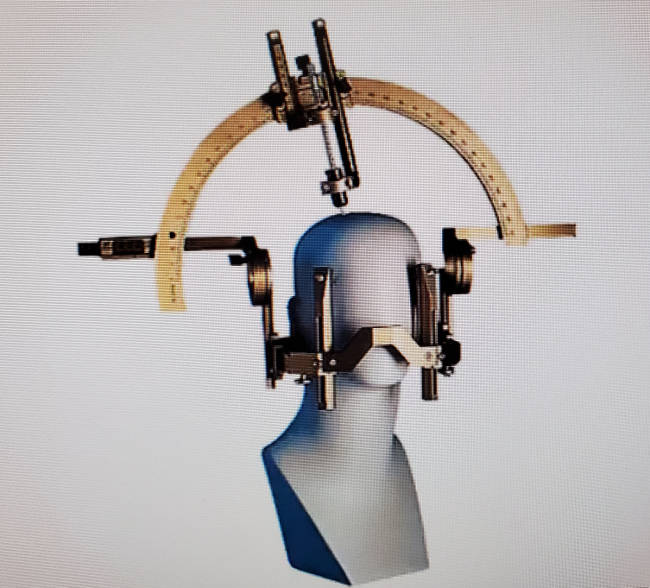
This surgical procedure embeds wires deep into the brain to connect an electrical power source to provide impulses to activate two basal ganglia regions of the brain (thalamus, subthalamic nucleus or globus pallidus) to improve motor symptoms such as tremors and dyskinesia. Inserting and targeting of the wire electrodes is planed using an magnetic resonance imaging (MRI) scan along with recordings of regions of the brain thought to be causing the problems. The impulse generator (neurostimulator) and battery are surgically implanted (typically under the collar bone or in the abdomen) as well. A controller is available to the patient so that it can be turned on or off. This surgery is typically reserved for those with advanced progression of Parkinson's Disease whose symptoms cannot be adequately controlled with medications. Deep Brain Stimulation (DBS) treats the patient by interrupting problematic electrical brain signals from the targeted area of the brain that are causing Parkinson's symptoms such as tremors. A successful surgery is usually followed by a reduction of medication and the medication side-effects.
The latest (2025) advance in DBS technology is "adaptive" or self-adjusting DBS which fine tunes, in real time, the level of electrical stimulation based on the needs of the patient. When medication kicks in, adaptive DBS senses this conditiion based on brain signals and reduces stimulation. When medications wear off, adaptive DBS will sense this condition and increase stimulation.
The implantation of DBS hardware (implantable pulse generator, battery, lead and lead extension) can be accomplished with the patients in either of two states:
- Awake: local anesthesia is used
- Asleep: this is a newer surgical procedure which is MRI guided
There are three DBS brain target options for Parkinson's which are referred to as:
- Thalamus: VIM Thalamus for essential tremor and tremor-predominant Parkinson's disease
- STN DBS: Subthalamic Nucleus Deep Brain Stimulation (more common - bilateral) more medication reduction, less‐frequent battery changes, improvements in rigidity
- GPI DBS: Globus Pallidus Internus Deep Brain Stimulation - more‐robust dyskinesia and dystonia suppression, easier programming, and greater flexibility in adjusting medications
Both regions are equally effective at tremor suppression. The GPI is the larger of the two brain regions (450mm3 vs 150mm3) requiring more power to stimulate but is an easier target for the surgeon, when installing lead wires, with a smaller chance of error. There can be unintended effects and behavioral changes when neighboring regions are accidentaly stimulated. For each target region there are two additional options, unilateral or bilateral.
DBS is also used to treat "essential tremors" by targeting other areas of the brain:
- VIM DBS: Ventral Intermediate (VIM) Nucleus of Thalamus Deep Brain Stimulation
- PSA DBS: Posterior Subthalamic Area Deep Brain Stimulation
Possible side effects and complications due to DBS include:
- Headache
- Confusion and problems with concentration
- Seizures
- Infection
- Stroke
- Difficulty with balance
- Difficulty with speech
- Mood changes and depression
- Tightning of muscles
- Double vision (ref Dr Hamedani)
- no or poor response to medication
- severe disability during best on time
- disability mainly from balance or gait problems
- depression or psychosis
- dementia
- patients with near Parkinson's syndromes: MSA, PSP, CBGD
Also see Subthalamic Nucleus Versus Globus Pallidus Internus Deep Brain Stimulation: Translating the Rematch Into Clinical Practice (2014)
DBS Vendors:- Medtronic: Percept - senses and records brain signal data for use in personalizing neurostimulator programming
- Abbott: Liberta DBS
- Boston Scientific: Vercise - uses 8 vvs 4 leads of traditional DBS systems
- Frame-based:
- Frameless:
- Renishaw: neuroguide - electrode positioning
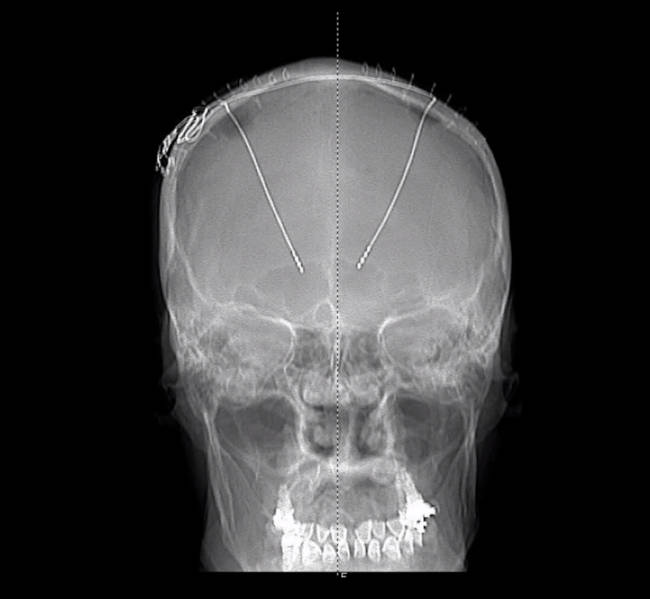 X-ray showing DBS leads routed deep into the brain
X-ray showing DBS leads routed deep into the brain
Pallidotomy:
Pallidotomy surgery seeks to damage an overactive globus pallidus to lessen the symptoms of Parkinson's disease (tremor, bradykinesia, and balance problems). The globus pallidus balances the excitatory action of the cerebellum and when this system is out of ballance, it can lead to tremors and jerky movement.
Thalamotomy:
Thalamotomy surgery seeks to damage an overactive thalamus to control the brain signals causing tremors. The celebrity actor Micheal j. Fox had a thalamotomy in 1998, to treat his Parkinson's tremors, as reported in Wikipedia.
A related FDA approved therapy has emerged for tremor dominant Parkinson's patients using ultrasound treatment instead of traditional surgery. It involves focused beams (less than 1 mm sq) of sound energy to heat and destroy a specific portion of the thalamus associated with the tremor (ventralis intermedius), guided by a real-time, high resolution MRI. The lesion is irreversible and not adjustable as Parkinson's advances. Known as "Magnetic Resonance-guided focused ultrasound" or MRgFUS, it avoids many of the risks of brain surgery such as infection, bleeding and stroke and is well tollerated by even frail patients and performed in a single session on an outpatient basis. Procedure lasts up to three hours. Side effects include trouble walking and balance. The system is manufactured by Insightec and is known as the "Exablate Neuro Platform" and requires no anesthesia, no incisions and no implanted hardware.

Magnetic Resonance-guided focused ultrasound (MRgFUS)
Pros:
- Potential to alleviate Parkinson's symptoms and reduce medication, thus reducing the side-effects of the medication (typically LDOPA dyskinesia and hallucinations).
Cons:
- Brain surgery has risk for infection, hemorrhaging, etc.